
Outer Hip Pain (GTPS)

Do you feel outer hip pain either during or after running? Does it also sometimes hurt when you cross your legs or sleep on your side? If so, read on as you may be suffering from GTPS..
GTPS stands for Greater Trochanteric Pain Syndrome (GTPS). The greater trochanter is the protuberance on the head of the thigh bone (femur); to find it your GT (as we will now refer to it) put your hands on your waist and then move them a fraction down – that’s your pelvis you’re now feeling. Keep moving downwards and eventually you will feel the top of your thigh bone sticking out. That’s your GT, and if touching it makes you jump you could well be suffering from GTPS.
What Causes GTPS?
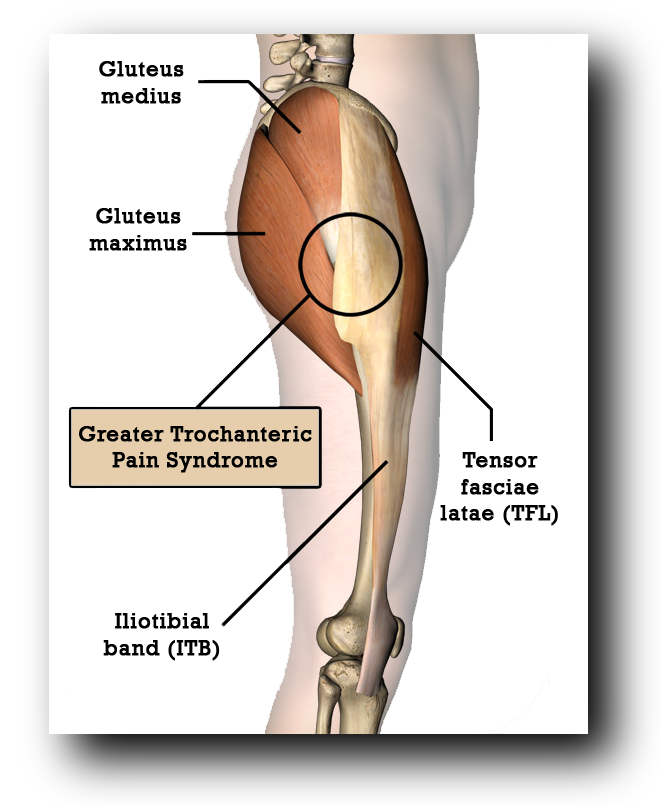
Sensitivity in this area is traditionally attributed to irritation of a bursa (a fluid-filled sac) that lies over the greater trochanter in order to protect the joint. However, more recent research (Long et al. 2013) suggests otherwise: in a study of 877 subjects with greater trochanteric pain, 700 did not have bursitis; instead, 438 had gluteal tendinosis (irritation of gluteus medius and/or gluteus minimus tendons) and 250 had a thickened iliotibial band (ITB). The tendons of the gluteus medius & minimus both attach to the greater trochanter and the ITB passes over it, as can be seen in the diagram.
The implication of GTPS being the result of aggravated tendons as opposed to an inflamed bursa is important in the sense that successful treatment & rehabilitation may well depend on:
1. Avoiding tendon compression as this could aggravate the tendons further
2. Ensuring a progressive resistance based exercise programme is put in place to strengthen the tendons and reduce system sensitivity.
3. Understanding that rest & anti-inflammatories are not likely to help if it’s not an inflammatory issue.
Tendons and Compression
Although tendons are magnificently tough structures that can handle incredible amounts of tension, research suggests they do always react as happily to compression. In the case of the gluteal tendons, movement of the leg towards the midline (adduction, e.g. when you cross your legs) can cause the iliotibial band (ITB) to compress the gluteal tendons, especially if the hip of the adducted leg is also flexed (brought up in front of you); tendons it would seem are particularly not fans of compression and tension at the same time.
In order to protect themselves, tendons react to compression by swelling. If the load demand is not reduced sufficiently (e.g. by suitable activity modification), the increase in tendon size can cause even more compression, leading to a self perpetuating cycle of ever increasing irritation. Tendon structure can then start to suffer with degeneration and potential tearing (rupture).
Pelvic Drop
Adduction of the leg can be caused by either moving the leg towards the midline (as in crossing your legs), or moving the midline towards the leg. The latter occurs when the opposite side of the hips falls, commonly referred to as pelvic drop. When you stand on one leg (as you do when running), one of the key roles of the glute medius & minimus is to stabilize the hip so that the opposite side of the pelvis (the non-weight bearing side) does not fall excessively. This can be seen in the diagram below.
On the left in the sketches (A) & (B), we see an illustration of a runner in ‘left leg swing phase’, i.e. the left foot has left the ground and is in the process of travelling forwards. The right leg is supporting the body weight with the right gluteus medius (highlighted) stabilizing the pelvis. In sketch (A), the left hip has remained more or less straight (in reality a drop of 4-5 degrees is generally expected) suggesting that the right gluteus medius is working well. However, in sketch (B) we see that the left hip has fallen, suggesting that the right gluteus medius is not working very well. The photo to the right of the sketches shows this same scenario in a real life runner.
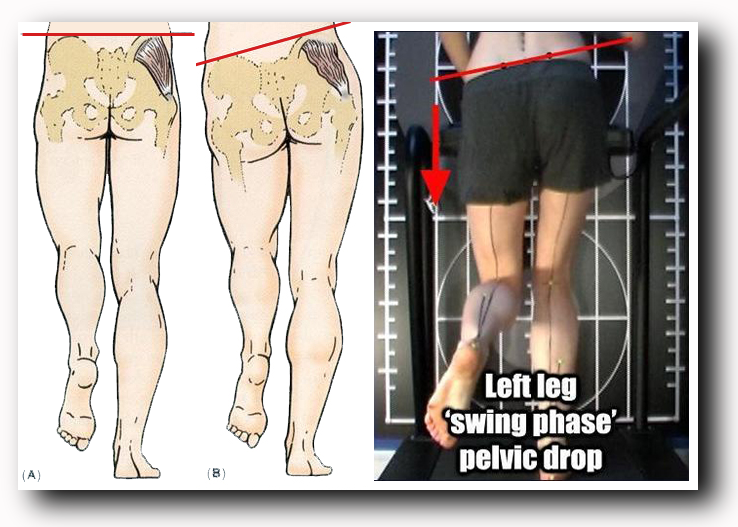
If we take a closer look at the right leg of the runner, we can see that because the left side of the pelvis has fallen, the right leg is in effect adducted. Combine this with the fact that the right hip is in a flexed (bent) position and we can begin to see how this posture during running can lead to aggravation of the glute medius and minimus tendons.
Symptoms of GTPS
For runners suffering from GTPS, the most painful moment of the run will be as in the image above, i.e. when the foot of the affected side lands and the body passes over it. Running on a slight slope (camber) can make things worse as it forces the leg into even more adduction. If left untreated, the pain can also start to affect you when you are not running. The most common symptom is hip pain when lying on the affected side as this increases compression on the tendon. Unfortunately, lying on the unaffected side can be just as uncomfortable as the top leg falls into an adducted (and often flexed) position. Putting a pillow between your thighs can often help. In some cases, sufferers may also experience pain when walking, especially if uphill or a flight of stairs, and when crossing the legs.
Management & Rehabilitation
If the GTPS is a tendon issue (it isn’t always), understanding how and why the above positions can further aggravate the situation is useful and necessary if you are going to succeed in allowing healing to occur. It will also help you choose a suitable rehabilitation program. If you have caught the aggravated tendon in the early stages, e.g. as a result of a recent sudden change in running frequency, intensity (especially hill work) or distance with no prior history of hip pain, the chances are the tendon is simply in an irritated state (referred to as ‘reactive’). If you have suffered the pain for longer and seen it gradually get worse, the actual state of the tendon may have been affected slightly (referred to as ‘degenerative’). It is important to differentiate between ‘reactive’ and ‘degenerative’ as rehab differs slightly for each.
In the case of a reactive tendon, you basically now have an extremely valuable opportunity to stop aggravating it and avoid harming tendon structure. The first step is to try and reduce activities that involve adduction, especially if they also involve flexion (lifting the leg up at the hip). Crossing the legs is a great example of exactly the two movements which we need to try to reduce. Amount of running will have to be decreased, especially if a gait assessment highlights the opposite hip does fall when taking weight on the symptomatic leg. How much you have to reduce these activities will depend on the extent of your symptoms.
A pain of 3 or 4 out of 10 is not generally anything to worry about but if a particular posture or movement (like running) is causing over a 5/10 then do try to avoid it for a while until your body becomes less sensitive and the tendon has had a chance to become less aggravated. Trying to run through a pain of over 5/10 is likely to make the situation worse and your rehab last longer.
“The amount of running you do will have to be decreased, especially if gait assessment highlights the opposite hip falling when taking weight on the symptomatic leg.”
As always with tendons, rest is only half of the story. It is vital that you start a program of suitable graded resistance exercises to help strengthen the tendon and reduce the threat to your system. The exercises chosen will initially need to avoid adduction and flexion, so the common ‘clam’ position for example is not a good choice. Instead, we tend to give out a side lying straight leg raise, with a pillow between the legs to ensure the affected leg on top does not move into an adducted position. We also make sure the leg on top is not flexed by holding it slightly behind the lower leg.
As far as sets and reps, we normally start with just holding the leg slightly up and away from the pillow for anything up to 30 seconds. This is called an isometric exercise and is generally regarded as a good starting point for loading a tendon. You may only be able to initially achieve a 2cm raise for 15 seconds but it is vital you don’t do too much too soon. As we mentioned above, if an exercise causes you a pain of about 3 or 4 out of 10 then that’s generally fine; in fact it’s normally a good sign that you are challenging the body sufficiently. However, if the exercise is causing over a 5/10 then that’s a sign that you are working too hard and need to make that exercise easier. It is not a case of no pain no gain. Once strength gains have been seen and symptoms have reduced slightly, we can progress to raising & lowering the leg (concentric & eccentric exercise).
From here, single leg balance exercises are a good place to move on to, but we need to make sure that the opposite hip is not falling because as we have seen this can aggravate the tendon. You can progress the single leg exercises by adding upper body rotation, slight knee bends, etc. A suitably experienced injury therapist will be able to ensure you choose the right exercises and progress them correctly as and when becomes appropriate.
Should I Stretch?
Treating an aggravated tendon is a perfect example of how stretching is not the answer. Trying to stretch the glutes or tensor fasciae latae (muscle at the top of the IT Band) can increase tendon compression and in doing so delay recovery and even make symptoms worse. Massage can help relax muscles, as can foam rolling but make sure you avoid allowing anyone or anything from applying direct pressure to the painful area.
In Summary
Pain at the top of the outer thigh when running could well be tendon related as opposed to down to bursa inflammation, and successful rehab will depend on treating it accordingly. I hope this article helps you if you are experiencing pain on the top outer thigh when running. As always, if in doubt get assessed by a professional and do let us know how you get on!
Have you ever suffered from outer hip pain when running? Was it diagnosed as GTPS? How did you deal with it Maybe you are a health professional yourself and would like to add something? Feel free to use the comments section below!
Related Posts
Five Best Ways For Runners To Warm Up
Want to know the five best ways for runners to warm up? What does the evidence say about Static stretching? How about Dynamic Stretching? What’s Dynamic Mobility? Prepare for surprises!

Hill Sprints for Novice Runners
For those relatively new to regular running, the notion of introducing maximal effort hill sprints is often met with concern over the possibility of over-training and encouraging injury. And yet, including one or two weekly hill sprint sessions into your training may well be safer than just knocking out long distances on flat ground.
Natural Equals Good – Logical Fallacy
A logical fallacy is something used in discussion / argument / marketing that sounds supportive but is actually based on a misassumption. For example, assuming something /someone must be good because it’s been around for many years is called an ‘appeal to antiquity’. They are worth recognising as soft tissue discussions are full of them.
0 Comments